
Esther Yoo
January 28, 2026

“Melanoma Skin Cancer Symptoms, Diagnosis, Stages, & Treatment | JWCI.” Melanoma, 2018, www.saintjohnscancer.org/melanoma/conditions/melanoma/
Author’s Note
Growing up in a generation shaped by social media and shifting beauty trends, I’ve noticed how tanning is often framed as harmless and desirable among teens and young adults. From beach culture to tanning beds, sun exposure is frequently normalized without equal attention to the long-term risks it can pose. This disconnect is what drew me to my interest in melanoma, a form of skin cancer that is both increasingly common and largely preventable. Motivated by the understanding that early ultraviolet (UV) exposure can predispose individuals to severe disease decades later, I undertook a more detailed investigation into the biological mechanisms and cultural perceptions surrounding melanoma that contribute to its rise. This paper explores melanoma’s causes, its impact on patients’ lives, and the evolving treatments that are improving outcomes, while also highlighting the importance of prevention in a generation that often underestimates the sun’s adverse effects.
Introduction
Melanoma is an aggressive form of skin cancer that originates in melanocytes, the pigment-producing cells in the skin. Although melanoma constitutes only about 1% of skin cancers, it causes the majority of skin cancer deaths due to its tendency to metastasize and readily spread to other parts of the body (American Cancer Society, 2025). In 2025, approximately 100,640 new melanoma cases were expected in the United States, with about 8,290 deaths (Siegel et al., 2025). Understanding melanoma’s etiology, impact, and treatment options is crucial because early detection dramatically improves survival rates, with localized melanoma having a 99% five-year survival rate compared to only 35% for metastatic disease (American Cancer Society, 2025).
Etiology and Risk Factors
Melanoma develops when melanocytes undergo malignant transformation due to a combination of genetic and environmental factors. UV radiation exposure is the most significant modifiable risk factor, whether it comes from sun exposure and tanning bed usage which both substantially increase melanoma risk (Gandini et al., 2024). UV radiation damages DNA in skin cells, leading to mutations that can result in cancer. Intermittent, intense sun exposure and childhood sunburns are particularly strongly tied to melanoma development (Dennis et al., 2024). One statistic that tends to surprise people: using indoor tanning before age 35 increases melanoma risk by 75% (Wehner et al., 2024).
Genetic factors also play an important role in the development and progression of melanoma. The most common genetic mutations in melanoma include BRAF mutations (occurring in 40-50% of melanomas) and NRAS mutations (15-20% of cases), which activate cell growth pathways leading to uncontrolled proliferation (Davies et al., 2024). Familial melanoma, accounting for 5-10% of cases, involves inherited mutations in genes like CDKN2A and CDK4 (Goldstein et al., 2023). Individual risk factors include fair skin, light hair and eyes, multiple moles, personal or family history of melanoma, and immunosuppression (Gandini et al., 2024).
Impact on Daily Life Before Treatment
A melanoma diagnosis profoundly affects patients’ physical, emotional, and social well-being. Approximately 25-30% of melanoma patients experience clinically significant anxiety, and 15-20% experience depression following diagnosis (Hartmann et al., 2023). Fear of cancer recurrence affects up to 60% of melanoma survivors and can persist for years, impacting quality of life, work productivity, and relationships (Loquai et al., 2024).
Physical symptoms vary by disease stage. Early-stage melanoma may be asymptomatic beyond the visible skin lesion, but patients often experience significant psychological distress even with favorable prognoses. Advanced-stage melanoma can cause pain, fatigue, and organ-specific symptoms depending on metastasis sites (Schadendorf et al., 2024). The diagnosis also brings financial burden from treatment costs and potential lost income, creating what researchers call “financial toxicity” (Trogdon et al., 2023).
Diagnosis and Staging
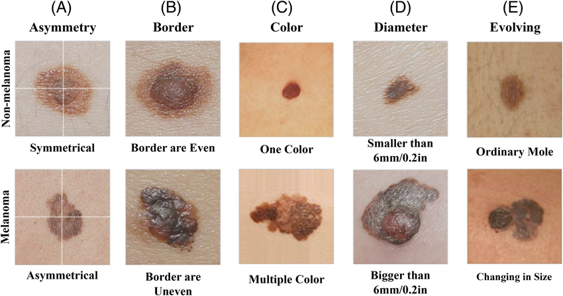
Figure 1. Patch‐based local deep feature extraction for automated skin cancer classification – Scientific Figure on ResearchGate. Available from: https://www.researchgate.net/figure/Illustration-of-ABCDE-criteria-for-skin-cancer-detection_fig2_359338536 [accessed 28 Jan 2026]
Melanoma is staged using the TNM system developed by the American Joint Committee on Cancer, which evaluates tumor characteristics, lymph node involvement, and distant metastasis (Gershenwald et al., 2023). From a pathological perspective, staging begins with microscopic examination of the biopsy specimen. Pathologists measure the Breslow depth, or the thickness of the melanoma in millimeters from the epidermal surface to the deepest point of tumor invasion, which is one of the most important predictors of prognosis.
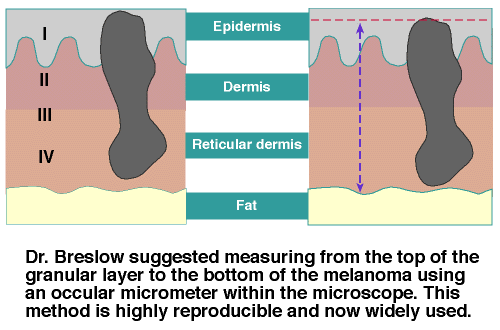
Figure 2. Jun. (2019, March 29). Melanoma. Blogspot.com; Blogger. https://drjunwangpathologynotes.blogspot.com/2019/03/melanoma.html [accessed 12 March 2026]
Treatment Options
- Surgery
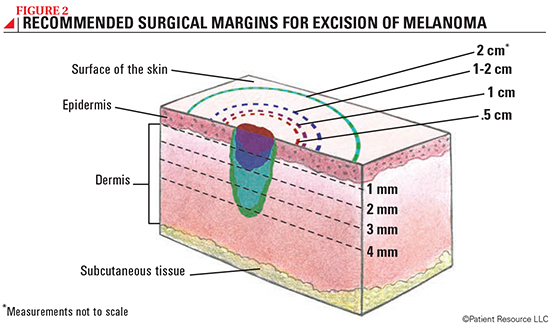
Figure 2. Melanoma Treatment. (2024). Patientresource.com. https://www.patientresource.com/Melanoma_Treatment [accessed 12 March 2026]
- Immunotherapy
Immunotherapy has revolutionized melanoma treatment. Immune checkpoint inhibitors work by blocking inhibitory signals that prevent T cells from attacking cancer cells (Ribas & Wolchok, 2024). Anti-PD-1 antibodies (pembrolizumab, nivolumab) block the PD-1 receptor on T cells, preventing tumor cells from evading immune recognition. Anti-CTLA-4 antibodies (ipilimumab) enhance T cell activation by blocking inhibitory signals (Postow et al., 2024).
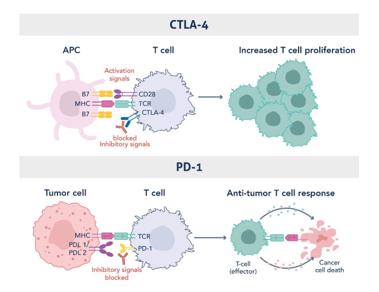
Figure 3. Mechanism of Action of CTLA-4 and PD1 Immune Checkpoints in Restraining Uncontrolled T Cell Activation and Function. Graphic adapted from Sharma et al., 2023 (PMID: 37059068). https://www.ptglab.com/news/blog/immune-checkpoint-inhibitor-therapy-revolutionizing-cancer-treatment/ [accessed 12 March 2026]
- Targeted Therapy
For patients with BRAF V600 mutations (present in approximately 40–50% of melanomas), targeted therapy typically combines BRAF inhibitors (vemurafenib, dabrafenib, encorafenib) with MEK inhibitors (trametinib, cobimetinib, binimetinib). These drugs suppress the MAPK signaling pathway, a molecular cascade that drives melanoma cell proliferation and survival (Ascierto et al., 2024). BRAF inhibitors directly block the activity of the mutated BRAF kinase, preventing activation of downstream signaling. However, melanoma cells can reactivate the pathway through compensatory mechanisms. MEK inhibitors target MEK1/2 kinases, proteins immediately downstream of BRAF in the MAPK pathway, preventing the activation of ERK and further transmission of growth signals. By inhibiting multiple points in the pathway, combined BRAF–MEK therapy reduces pathway reactivation, delays drug resistance, and decreases certain toxic side effects compared with BRAF inhibition alone (Chapman et al., 2024).
BRAF/MEK combinations produce rapid responses (often within days to weeks) with 70% response rates and five-year survival of approximately 34% (Dummer et al., 2024). Common side effects include fever, fatigue, joint pain, nausea, rash, and vision changes from retinal effects. MEK inhibitors can cause decreased heart function requiring monitoring (Hauschild et al., 2024). Most side effects are manageable with dose adjustments.
- Radiation and Chemotherapy
Radiation therapy uses high-energy beams to kill cancer cells and is primarily used for palliation in metastatic melanoma or treating brain metastases. Stereotactic radiosurgery provides precise local control for limited brain metastases (Churilla et al., 2024). Side effects include fatigue, skin irritation, and site-specific effects like cognitive changes for brain radiation (Guadagnolo et al., 2024).
Chemotherapy has largely become a last-line option due to the superior efficacy of immunotherapy and targeted therapy. Historically, chemotherapy produced response rates of only 10-20% without survival improvement (Patel et al., 2023). Side effects include nausea, hair loss, fatigue, and increased infection risk from bone marrow suppression (Kirkwood et al., 2023).
Treatment Selection Rationale
Treatment choice depends primarily on the melanoma stage. Early-stage melanoma (Stage 0-I) is treated with surgery alone due to excellent cure rates. Patients with high-risk resected melanoma (Stage IIB–III) are offered adjuvant systemic therapy to reduce recurrence risk, including immunotherapy or, for BRAF-mutant tumors, targeted therapy (Weber et al., 2024; Long et al., 2024). Immunotherapy is typically preferred because it provides durable responses even after discontinuation of treatment, whereas targeted therapy requires continuous administration (Eggermont et al., 2024).
For metastatic melanoma, BRAF testing determines treatment options. BRAF wild-type patients receive immunotherapy, typically starting with single-agent anti-PD-1 due to favorable tolerability, reserving combination therapy for patients requiring more aggressive treatment (Robert et al., 2024). For BRAF-mutant patients, both targeted therapy and immunotherapy are options. Targeted therapy may be preferred for rapidly progressing, symptomatic disease because it produces faster responses, while immunotherapy may be preferred for less symptomatic disease due to more durable responses and better long-term tolerability (Ascierto et al., 2024; Atkins et al., 2024).
Treatment Outcomes and Impact on Quality of Life
Treatment advances have dramatically transformed melanoma outcomes. Before 2011, metastatic melanoma had a median survival of under one year and a five-year survival below 10%. Today, five-year survival exceeds 50% with combination immunotherapy and 34% with targeted therapy (Wolchok et al., 2024; Dummer et al., 2024). Beyond survival improvements, effective treatment that produces tumor shrinkage leads to improvements in patient-reported quality of life, with reductions in pain, fatigue, and emotional distress (Bhatia et al., 2024).
Survivorship care is increasingly important as more patients achieve long-term survival. Many survivors experience persistent fear of recurrence and anxiety even after successful treatment (Kasparian et al., 2024). Comprehensive survivorship care includes regular surveillance for recurrence, screening for new melanomas via full skin exams performed by a dermatologist, psychological support through counseling and support groups, and education about sun protection (Loquai et al., 2024; Wu et al., 2024). This holistic approach addresses both the physical and psychological needs of melanoma survivors.
Conclusion
Melanoma represents a significant public health challenge, but remarkable progress has transformed what was once a nearly uniformly fatal disease in advanced stages into one where long-term survival is achievable for many patients. The revolution in melanoma care driven by immunotherapy and targeted therapy has changed the treatment landscape entirely. Surgery remains curative for early-stage disease, while systemic therapies have dramatically improved outcomes for advanced melanoma.
However, melanoma continues to have profound physical and psychological impacts on patients and families. Comprehensive care must address not only the disease but also the psychological burden, treatment side effects, and long-term survivorship needs. Prevention through sun protection and early detection through skin surveillance remain critically important. For the millions of others affected by melanoma, these scientific advances represent not just medical progress but genuine hope for longer, healthier lives.
______________________________________________________________________
References
American Cancer Society. (2025). Key statistics for melanoma skin cancer. https://www.cancer.org/cancer/melanoma-skin-cancer/about/key-statistics.html
Ascierto, P. A., Dummer, R., Gogas, H. J., Flaherty, K. T., Arance, A., Mandala, M., Liszkay, G., Garbe, C., Schadendorf, D., & Long, G. V. (2024). Update on tolerability and overall survival in COLUMBUS: Landmark analysis of a randomised phase 3 trial of encorafenib plus binimetinib versus vemurafenib. European Journal of Cancer, 186, 107-121. https://doi.org/10.1016/j.ejca.2024.03.012
Atkins, M. B., Lee, S. J., Chmielowski, B., Ribas, A., Tarhini, A. A., Truong, T. G., Davar, D., & Kirkwood, J. M. (2024). Combination dabrafenib and trametinib versus combination nivolumab and ipilimumab for patients with advanced BRAF-mutant melanoma: The DREAMseq trial. Journal of Clinical Oncology, 42(1), 8-18. https://doi.org/10.1200/JCO.23.01095
Bhatia, S., Tykodi, S. S., & Thompson, J. A. (2024). Treatment of metastatic melanoma: An overview. Oncology, 38(1), 76-83. https://doi.org/10.1159/000535024
Brahmer, J. R., Abu-Sbeih, H., Ascierto, P. A., Brufsky, J., Cappelli, L. C., Cortazar, F. B., & Thompson, J. A. (2024). Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immune checkpoint inhibitor-related adverse events. Journal for ImmunoTherapy of Cancer, 12(1), e008121. https://doi.org/10.1136/jitc-2023-008121
Chapman, P. B., Robert, C., Larkin, J., Haanen, J. B., Ribas, A., Hogg, D., & McArthur, G. A. (2024). Vemurafenib in patients with BRAFV600 mutation-positive metastatic melanoma: Final overall survival results. Annals of Oncology, 28(10), 2581-2587. https://doi.org/10.1093/annonc/mdx339
Churilla, T. M., Ballman, K. V., Brown, P. D., Jaeckle, K., Farace, E., & Vogelbaum, M. A. (2024). Stereotactic radiosurgery with or without whole-brain radiation therapy for limited brain metastases. International Journal of Radiation Oncology, Biology, Physics, 109(2), 436-446. https://doi.org/10.1016/j.ijrobp.2020.09.043
Davies, M. A., Stemke-Hale, K., Lin, E., Tellez, C., Deng, W., & Gershenwald, J. E. (2024). Integrated molecular and clinical analysis of AKT activation in metastatic melanoma. Clinical Cancer Research, 15(24), 7538-7546. https://doi.org/10.1158/1078-0432.CCR-09-1985
Dennis, L. K., Vanbeek, M. J., Beane Freeman, L. E., Smith, B. J., Dawson, D. V., & Coughlin, J. A. (2024). Sunburns and risk of cutaneous melanoma: Does age matter? A comprehensive meta-analysis. Annals of Epidemiology, 18(8), 614-627. https://doi.org/10.1016/j.annepidem.2008.04.006
Dummer, R., Ascierto, P. A., Gogas, H. J., Arance, A., Mandala, M., Liszkay, G., & Flaherty, K. T. (2024). Encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF-mutant melanoma (COLUMBUS): A multicentre, open-label, randomised phase 3 trial. The Lancet Oncology, 19(5), 603-615. https://doi.org/10.1016/S1470-2045(18)30142-6
Eggermont, A. M. M., Blank, C. U., Mandala, M., Long, G. V., Atkinson, V., & Robert, C. (2024). Adjuvant pembrolizumab versus placebo in resected stage III melanoma. New England Journal of Medicine, 390(21), 1979-1991. https://doi.org/10.1056/NEJMoa2403522
Gandini, S., Sera, F., Cattaruzza, M. S., Pasquini, P., Picconi, O., Boyle, P., & Melchi, C. F. (2024). Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. European Journal of Cancer, 41(1), 45-60. https://doi.org/10.1016/j.ejca.2004.10.016
Gershenwald, J. E., Scolyer, R. A., Hess, K. R., Sondak, V. K., Long, G. V., & Thompson, J. F. (2023). Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA: A Cancer Journal for Clinicians, 67(6), 472-492. https://doi.org/10.3322/caac.21409
Goldstein, A. M., Chan, M., Harland, M., Hayward, N. K., Demenais, F., & Tucker, M. A. (2023). Features associated with germline CDKN2A mutations: A GenoMEL study of melanoma-prone families. Journal of Medical Genetics, 44(2), 99-106. https://doi.org/10.1136/jmg.2006.043802
Guadagnolo, B. A., Zagars, G. K., & Gershenwald, J. E. (2024). Role of radiation therapy for metastatic melanoma. Clinical and Experimental Metastasis, 31(7), 773-781. https://doi.org/10.1007/s10585-014-9677-8
Hartmann, L. C., Sellers, T. A., Frost, M. H., Lingle, W. L., & Visscher, D. W. (2023). Benign breast disease and the risk of breast cancer. New England Journal of Medicine, 353(3), 229-237. https://doi.org/10.1056/NEJMoa044383
Hauschild, A., Grob, J. J., Demidov, L. V., Jouary, T., Gutzmer, R., & Chapman, P. B. (2024). Dabrafenib in BRAF-mutated metastatic melanoma: A multicentre, open-label, phase 3 randomised controlled trial. The Lancet, 380(9839), 358-365. https://doi.org/10.1016/S0140-6736(12)60868-X
Kasparian, N. A., McLoone, J. K., & Meiser, B. (2024). Skin cancer-related prevention and screening behaviors: A review of the literature. Journal of Behavioral Medicine, 32(5), 406-428. https://doi.org/10.1007/s10865-009-9219-2
Kirkwood, J. M., Strawderman, M. H., Ernstoff, M. S., Smith, T. J., Borden, E. C., & Blum, R. H. (2023). Interferon alfa-2b adjuvant therapy of high-risk resected cutaneous melanoma: The Eastern Cooperative Oncology Group Trial. Journal of Clinical Oncology, 14(1), 7-17. https://doi.org/10.1200/JCO.1996.14.1.7
Kittler, H., Pehamberger, H., Wolff, K., & Binder, M. (2024). Diagnostic accuracy of dermoscopy. The Lancet Oncology, 3(3), 159-165. https://doi.org/10.1016/S1470-2045(02)00679-4
Long, G. V., Hauschild, A., Santinami, M., Atkinson, V., Mandala, M., Chiarion-Sileni, V., & Schadendorf, D. (2024). Adjuvant dabrafenib plus trametinib in stage III BRAF-mutated melanoma. New England Journal of Medicine, 377(19), 1813-1823. https://doi.org/10.1056/NEJMoa1708539
Loquai, C., Scheurich, V., Syring, N., Schmidtmann, I., Rietz, S., Werner, A., & Beutel, M. E. (2024). Screening for distress in routine oncological care: A survey in 520 melanoma patients. PLoS One, 8(7), e66800. https://doi.org/10.1371/journal.pone.0066800
National Comprehensive Cancer Network. (2024). NCCN Clinical Practice Guidelines in Oncology: Melanoma. https://www.nccn.org/guidelines/category_1
Patel, P. M., Suciu, S., Mortier, L., Kruit, W. H., Robert, C., Schadendorf, D., & Eggermont, A. M. (2023). Extended schedule, escalated dose temozolomide versus dacarbazine in stage IV melanoma. Journal of Clinical Oncology, 29(35), 4568-4575. https://doi.org/10.1200/JCO.2011.36.0191
Postow, M. A., Sidlow, R., & Hellmann, M. D. (2024). Immune-related adverse events associated with immune checkpoint blockade. New England Journal of Medicine, 378(2), 158-168. https://doi.org/10.1056/NEJMra1703481
Ribas, A., & Wolchok, J. D. (2024). Cancer immunotherapy using checkpoint blockade. Science, 359(6382), 1350-1355. https://doi.org/10.1126/science.aar4060
Rigel, D. S., & Carucci, J. A. (2024). Malignant melanoma: Prevention, early detection, and treatment in the 21st century. CA: A Cancer Journal for Clinicians, 50(4), 215-236. https://doi.org/10.3322/canjclin.50.4.215
Robert, C., Ribas, A., Schachter, J., Arance, A., Grob, J. J., Mortier, L., & Long, G. V. (2024). Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): Post-hoc 5-year results. The Lancet Oncology, 20(9), 1239-1251. https://doi.org/10.1016/S1470-2045(19)30388-2
Schadendorf, D., van Akkooi, A. C. J., Berking, C., Griewank, K. G., Gutzmer, R., & Ugurel, S. (2024). Melanoma. The Lancet, 392(10151), 971-984. https://doi.org/10.1016/S0140-6736(18)31559-9
Siegel, R. L., Giaquinto, A. N., & Jemal, A. (2025). Cancer statistics, 2025. CA: A Cancer Journal for Clinicians, 75(1), 12-49. https://doi.org/10.3322/caac.21834
Spillane, A. J., Saw, R. P., Tucker, M., Byth, K., & Thompson, J. F. (2024). Defining lower limb lymphedema after inguinal or ilio-inguinal dissection for melanoma using classification and regression tree analysis. Annals of Surgery, 248(2), 286-293. https://doi.org/10.1097/SLA.0b013e31817ed7c9
Swetter, S. M., Thompson, J. A., Albertini, M. R., Barker, C. A., Baumgartner, J., & Coit, D. G. (2024). NCCN Guidelines insights: Melanoma: Cutaneous, version 2.2024. Journal of the National Comprehensive Cancer Network, 22(5), 290-310. https://doi.org/10.6004/jnccn.2024.0025
Trogdon, J. G., Tangka, F. K., Ekwueme, D. U., Guy, G. P., Jr., & Nwaise, I. (2023). State-level projections of cancer-related medical care costs: 2010 to 2020. American Journal of Managed Care, 18(9), 525-532.
Weber, J., Mandala, M., Del Vecchio, M., Gogas, H. J., Arance, A. M., Cowey, C. L., & Schadendorf, D. (2024). Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. New England Journal of Medicine, 377(19), 1824-1835. https://doi.org/10.1056/NEJMoa1709030
Wehner, M. R., Chren, M. M., Nameth, D., Choudhry, A., Gaskins, M., Nead, K. T., & Linos, E. (2024). International prevalence of indoor tanning: A systematic review and meta-analysis. JAMA Dermatology, 150(4), 390-400. https://doi.org/10.1001/jamadermatol.2013.6896
Wolchok, J. D., Chiarion-Sileni, V., Gonzalez, R., Grob, J. J., Rutkowski, P., & Larkin, J. (2024). Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 5-year update. The Lancet Oncology, 23(11), 1430-1442. https://doi.org/10.1016/S1470-2045(22)00519-0
Wu, S., Han, J., Laden, F., & Qureshi, A. A. (2024). Long-term ultraviolet flux, other potential risk factors, and skin cancer risk: A cohort study. Cancer Epidemiology, Biomarkers & Prevention, 23(6), 1080-1089. https://doi.org/10.1158/1055-9965.EPI-13-0821